Ziftomenib triplet shows 87% ORR in venetoclax-naive R/R AML
Kura Oncology and its Japanese partner Kyowa Kirin have published updated results from the KOMET-007 Phase 1a/b trial in the journal Blood, reporting that the investigational triplet of ziftomenib, venetoclax, and azacitidine produced deep and durable responses in adults with relapsed or refractory NPM1-mutated acute myeloid leukaemia (AML). The data, drawn from 64 response-evaluable patients as of a January 2026 data cutoff, represent the most mature readout of this combination to date.
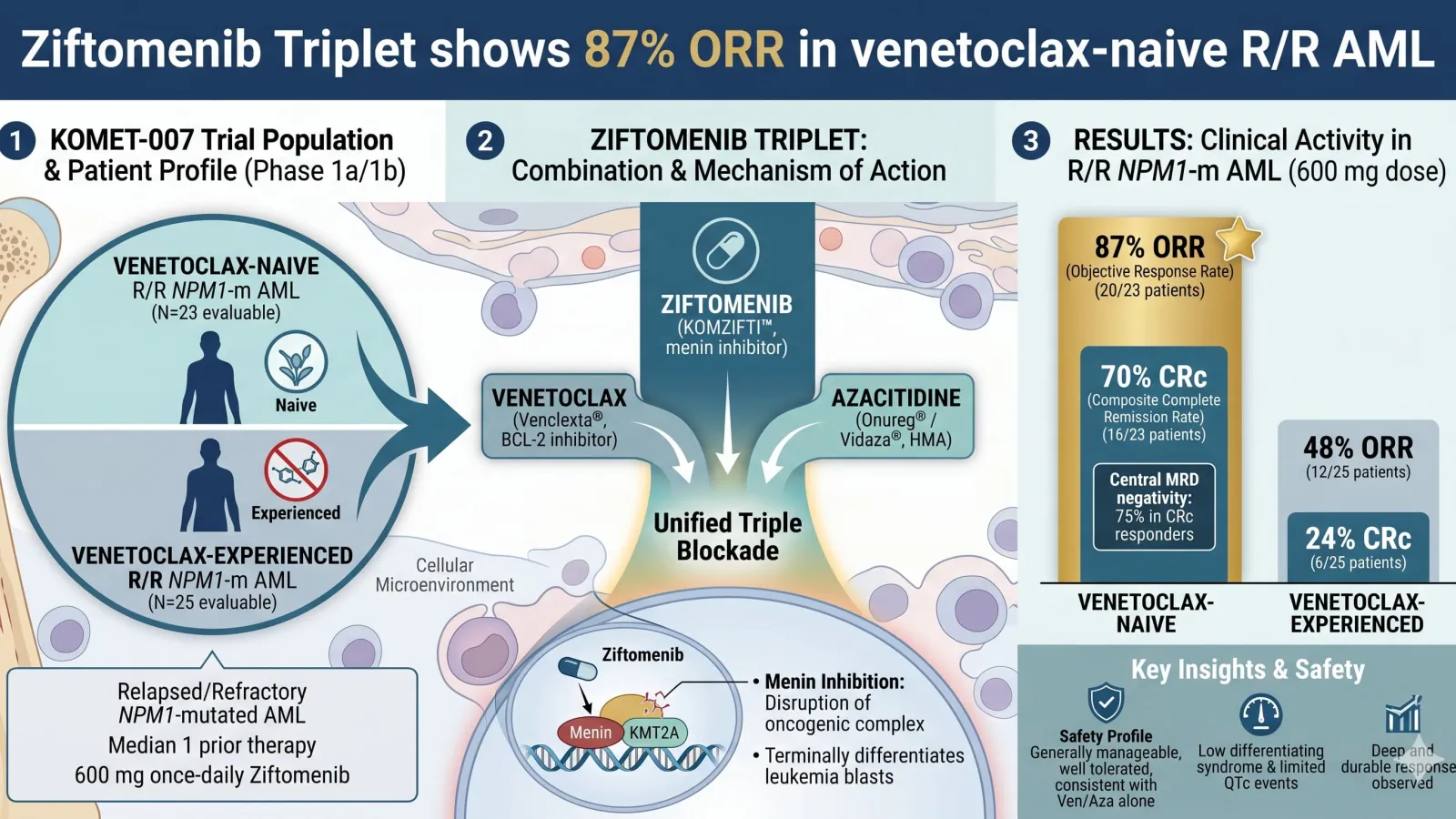
At the recommended 600 mg once-daily ziftomenib dose, venetoclax-naïve patients achieved an 87% objective response rate and a 70% composite complete remission (CRc) rate. Three-quarters of CRc responders in that group were centrally confirmed as measurable residual disease (MRD) negative — a marker of molecular depth that carries prognostic weight in AML. Median overall survival had not been reached after a median follow-up of 10.7 months. In venetoclax-experienced patients, a harder-to-treat population, the ORR was 48% and the CRc rate was 24%, with a median OS of 7.4 months — a clinically meaningful result in a setting where prior venetoclax exposure typically blunts subsequent responses.
Clinical significance
Eunice S. Wang, Chief of Leukaemia at Roswell Park Comprehensive Cancer Center and co-first senior author of the publication, noted that outcomes with venetoclax-based regimens in the relapsed/refractory NPM1-mutant setting "remain suboptimal," adding that the KOMET-007 results were notable for "the depth and durability of response observed with the investigational three-drug combination." The safety profile was broadly manageable: differentiation syndrome — a boxed-warning risk for ziftomenib as monotherapy — occurred in only 3% of patients (2/67) across all dose levels, attributed to a protocol-specified staggered dosing schedule in which ven/aza is administered before menin inhibition begins. A single case of ziftomenib-related QTc prolongation was reported and resolved without dose change.
Mollie Leoni, Chief Medical Officer of Kura Oncology, said the data "strengthen the case for ziftomenib as a backbone in NPM1-mutant AML" and pointed to ongoing randomised studies in newly diagnosed disease as the next frontier.
Market context and competitive landscape
Ziftomenib, marketed as KOMZIFTI, received FDA approval as monotherapy for R/R NPM1-mutated AML in 2025, making it one of the first approved menin inhibitors. The broader menin inhibitor class has attracted significant attention; revumenib (Syndax Pharmaceuticals) is also approved in the R/R AML setting and is being evaluated in combination regimens, creating a competitive dynamic that will intensify as both programmes move into earlier lines of therapy and newly diagnosed disease. The outcome in venetoclax-experienced patients is an important differentiating data point, given the rapid uptake of ven/aza as a front-line standard of care: most patients arriving in the relapsed setting will have prior venetoclax exposure, making that 48% ORR a more commercially relevant benchmark than the venetoclax-naïve figures.
Kura and Kyowa Kirin are pursuing two pivotal Phase 3 trials — KOMET-017 — in newly diagnosed NPM1-mutated and KMT2A-rearranged AML. Positive randomised data from those studies would be required before ziftomenib-based combinations could seek regulatory approval beyond the current monotherapy label. The EMA has not yet granted approval for ziftomenib in any indication, meaning European commercial optionality remains contingent on a separate regulatory filing. Investors will be watching KOMET-017 enrolment timelines and any interim futility analyses as the programme's critical near-term milestones.